Man overboard whilst checking pilot ladder height
A Bosun fell overboard while checking whether the pilot ladder was rigged with the required height of one metre above the waterline.
What happened?

Photo #1 - Example of a pilot ladder hauled by a "tripping line".
The pilot ladder was hanging over-side in a U-shape. The Rubber steps (bottom steps) were lifted by means of a tripping line and the rope end tied to the railing.
At about dawn, the anchor party consisting of the Chief Officer, the Bosun and the Deck Cadet were at the forecastle deck to weigh the anchor for departure from the anchorage.
The Bosun had overheard the Master instructing the Chief Officer to adjust the height of the pilot ladder to one metre above the waterline. After heaving up the anchor, the Bosun then proceeded to the pilot ladder station to commence adjustment of the pilot ladder. Coming from the anchor station, he was attired in a helmet, safety boots, torchlight, walkie-talkie. He did not put on the work vest and safety harness that were placed at the pilot ladder station.
The Deck Cadet squared up the forecastle deck and went to the pilot ladder station to assist the Bosun. He too did not put on the work vest and safety harness.
The Chief Officer walked back to the accommodation block through the elevated central walkway, briefly stopping at the starboard manifold to see the progress of the work carried out by the Bosun. He did not stay to supervise the job till completion and did not intervene despite seeing that the Bosun was working without donning the safety vest/harness.
The pilot ladder was hanging over-side in a U-shape. The Rubber steps (bottom steps) were lifted by means of a tripping line and the rope end tied to the railing.

Photo #2 - Positions of the Chief Officer, Bosun and the Deck Cadet at 0637H
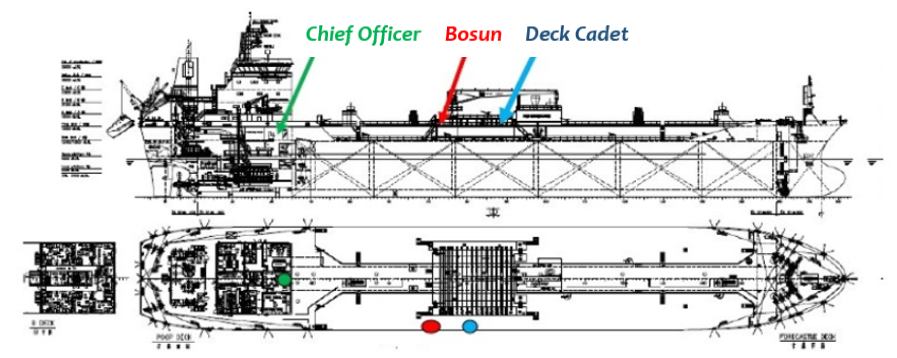
Photo #3 - Positions of the Chief Officer, Bosun and the Deck Cadet at 0639H

Photo #4 - Re-enactment of positions of the Bosun and the Deck Cadet at 0639H before the man overboard incident
While both of them were checking the height of the pilot ladder, the Deck Cadet heard a shout from the Bosun; and when he turned, the Bosun was seen falling into the sea.
Shocked and petrified by how fast the struggling Bosun was drifting away from the ship, the Deck Cadet did not throw the man-overboard lifebuoy towards the Bosun. Instead, he advanced aft and visually tracked the Bosun in the water so as not to lose sight of him while hastily informing the bridge of this accident using his walkie-talkie.
The Master who received the alert at the bridge was initially doubtful about the identity of the caller. The cadet did not identify himself clearly nor communicate the situation coherently. After establishing that one of his crew had indeed fallen overboard, the Master enlisted the assistance of the Mooring Master to deploy the nearby tugs. He did not order the release of the Bridge Wing's Man-overboard Marker Buoy, ring the emergency station, nor initiate the Man-overboard manoeuvre.
Within fifteen minutes, one of the responding tugs managed to locate and retrieve the Bosun from the water. However, despite the valiant efforts of the Tug Master, he was unable to revive the Bosun.
The autopsy report revealed drowning as the cause of death. The report also revealed that the Bosun had suffered some external injuries on his scalp, right lower back, left elbow, left thigh and below the left knee. No fractures were detected.
Why did it happen?
- The Bosun, coming directly from the anchor station, was dressed for anchor work. He did not put on the harness/safety vest for working at/or near ship side where there is a risk of falling overboard.
Lesson learnt: Always ensure and remind the crew to don the appropriate Personal Protective Equipment when performing ship's tasks. - There was no responsible officer overseeing the shipboard task; the Chief Officer went back to the ship's office before the task was completed.
Lesson learnt: It is important to have a responsible person to oversee and supervise a critical but routine shipboard task. This person can provide timely and resolute intervention when noticing Unsafe Acts carried out under Unsafe Conditions. - The method of ascertaining the height of the pilot ladder was unsafe and the Bosun had fallen overboard while doing so.
Lesson learnt: A safer method of ascertaining the height of the pilot ladder would be to first determine the vessel's freeboard and lower only the required length of the pilot ladder. This method would entail pre-marking the pilot ladder at suitable intervals to denote lengths, thus dispensing with the need for the crew to look over-side to ascertain the height of the pilot ladder above the waterline. -
The Deck Cadet, in his petrified state, did not release the lifebuoy to the Bosun struggling in the water. His last Man-Overboard (MOB) Drill was when he was serving on board his previous ship and he had not participated in any MOB drill on this ship. This could have explained his petrified state and ended up not releasing the lifebuoy to the Bosun.
Lesson learnt: It is important to provide training to deal with shipboard situations so that actions taken should be second nature to the crew onboard. A lack of training and a lack of awareness were among the factors that led to the inadequate handling of the situation at the first instance and the poor communication relayed to the master when the accident happened.
Recommendations
- Vessel's ISM Managers should review the methodology of rigging and ascertaining the height of pilot ladder above the waterline, and put in place mitigating measures against the risk of crew falling overboard when performing such tasks.
- In the absence SOLAS requirements for pre-determined frequency of a MOB drill, it would be desirable for such a drill to be conducted more frequently such as in conjunction with the launching of rescue boat or lifeboat (as appropriate).
- Owners, ISM Managers and Masters of Singapore registered ships are encouraged to plan man overboard drill in conjunction with the launching of rescue boat or lifeboat (as appropriate) for ensuring effective crew familiarisation with actions to be taken in a man overboard situation.
- Although not contributory to the death, but recognising the potential for an undesirable incident or occurrence, vessels are reminded to review the use of "tripping" or "retrieval" line on board taking guidance from IMO document A27/Res.1045; 2.1.5 "When a retrieval line is considered necessary to ensure the safe rigging of a pilot ladder, the line should be fastened at or above the last spreader step and should lead forward. The retrieval line should not hinder the pilot nor obstruct the safe approach of the pilot boat."